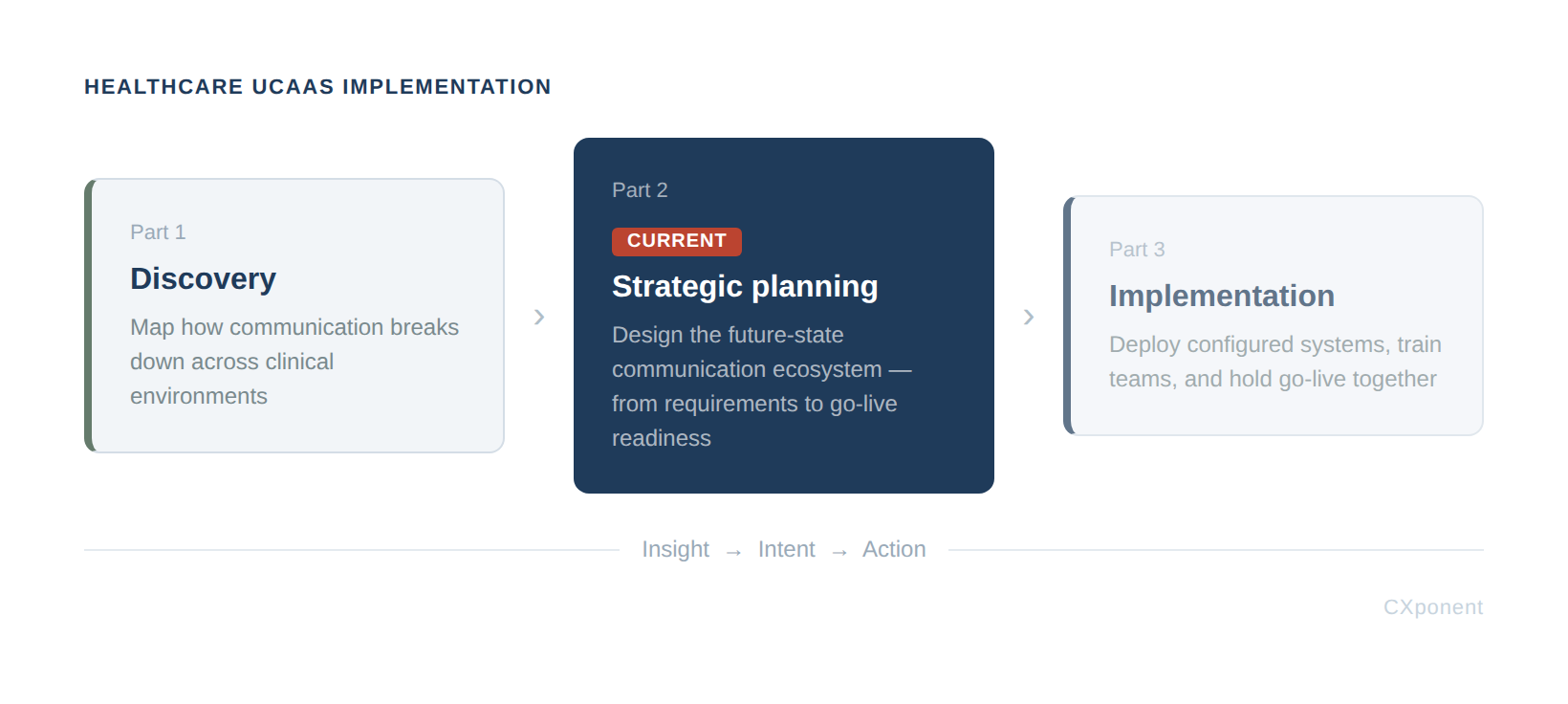
Implementing Healthcare UCaaS, Part 2: From Discovery to Strategic Planning

Implementing Healthcare UCaaS, Part 1 focused on Discovery, which provides vital visibility into how communication actually breaks down across clinical and operational environments, where workarounds introduce risk into patient care. But insight without structure is just awareness, and awareness alone doesn't improve anything.
The value of Discovery is only realized when its findings are translated into a clear, intentional plan for communication moving forward. This is the pivot point where many UCaaS initiatives drift. Organizations often leave Discovery with a long list of requirements but lack the structured framework to build a cohesive strategy, leading to reactive planning. Decisions start favoring platform capabilities over clinical needs, and workflows are adapted to fit technology instead of the other way around. The consequences of this drift are measurable:
Per CRICO, communication failures account for nearly 30 percent of malpractice claims. The failure is not clinical judgment, but information transfer being delayed, incomplete, or absent.
Phase II: Strategic Planning exists to prevent this by translating raw discovery data into purposeful design.
This doesn't need to be final. It needs to be functional. Refine it as the rollout matures and real usage patterns emerge.
Last, name one person responsible for channel discipline post-go-live before configuration begins. Not a committee — one person. Governance doesn't need to be elaborate at this stage; it needs to exist. Someone to hold the line, absorb the edge cases, and make the calls that keep the design from drifting. That role can evolve. Right now, it just needs to be filled.
Phase II: Strategic Planning
Where vision becomes action and communication strategy takes shape.
Strategic planning often gets mistaken for tool selection, but that’s not where real transformation begins. It starts with a clear vision of what communication should enable.
Communication in healthcare serves as more than just an operational function; it is fundamental to achieving clinical results. Successful strategic planning shifts the focus from accumulating features and platforms to fostering an environment where decision-making is prompt, coordination is fluid, and patient care is reliably sustained. Moving beyond a tool-centric approach toward an outcome-driven framework is what truly characterizes effective strategy.
To get there, organizations must anchor their approach in a few non-negotiable principles:
- Patient safety comes first and communication should reduce risk, not introduce it.
- Speed matters, especially when time-sensitive information can impact care.
- Reliability is critical; messages must reach the right people, every time, without fail.
None of this works without alignment. Clinical, operational, and IT leaders all play a role in shaping how communication flows across the organization. When these groups operate in silos, fragmentation follows. But when they align in a shared vision, communication becomes a unifying force rather than a point of friction.
Ultimately, the objective is purposeful design. Organizations move away from merely stacking new technologies on top of legacy systems and instead develop a unified communication ecosystem. This creates a framework that is both dependable and scalable, specifically engineered to enhance the experience for clinicians and patients alike.
Defining Requirements: Must-Have vs. Nice-to-Have
With a shared vision in place, strategic planning becomes concrete.. Principles like patient safety, speed, and reliability now have to translate into tangible decisions about what the communication ecosystem must do and what it doesn't need to do yet. This is where many organizations stumble.
Discovery typically produces a sprawling list of requests from clinicians, operations, and IT. Without disciplined prioritization, every item gets stamped "essential" and when everything is essential, nothing truly is. Scope expands, timelines slip, and the original purpose of the initiative gets diluted by competing priorities. In healthcare, scope creep doesn't just delay projects. It delays the outcomes communication is meant to support.
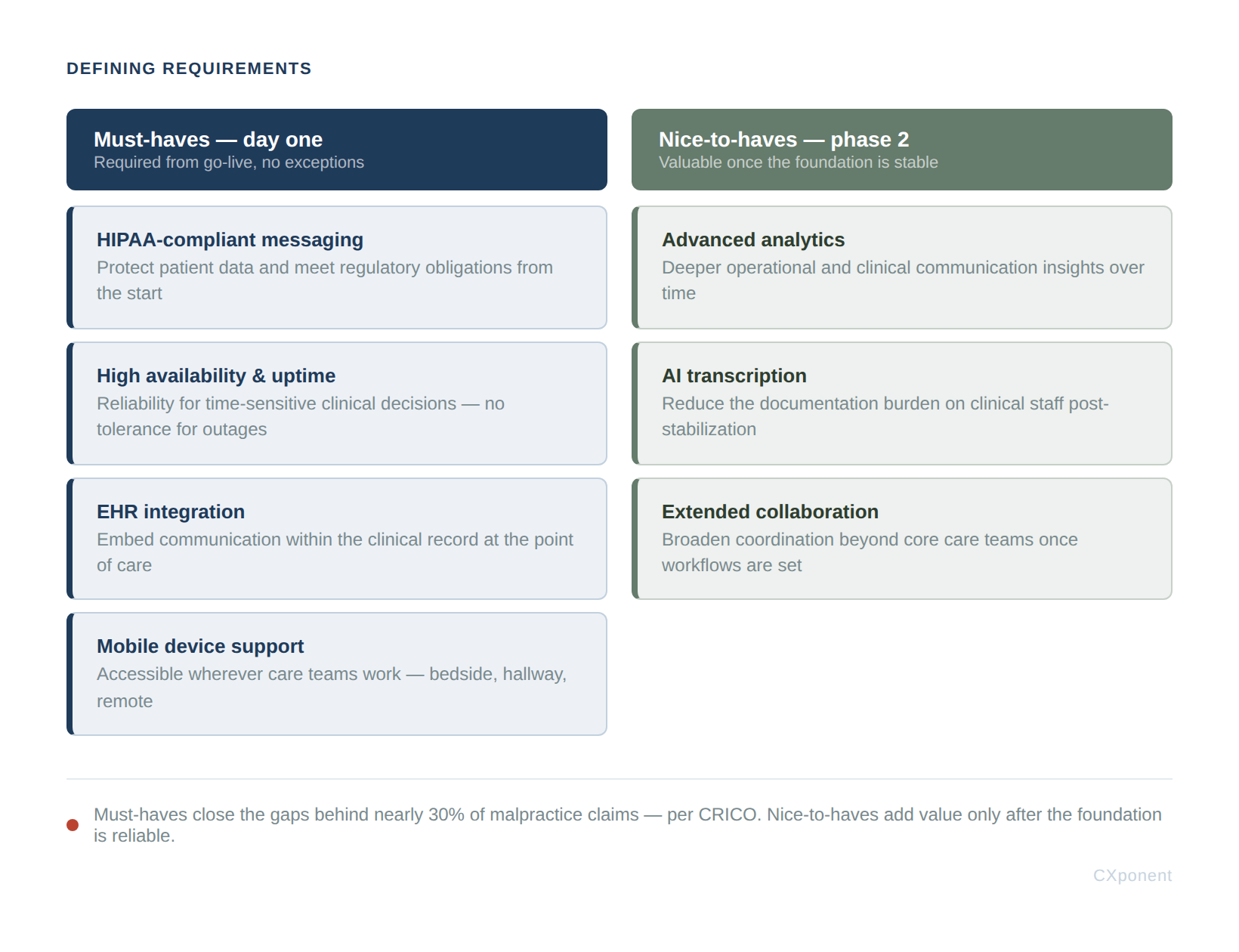
Must-Haves: The Critical Capabilities
Must-haves are the baseline capabilities that clinical work depends on and required from day one, no exceptions.
HIPAA-Compliant Messaging: Protect patient information and meet regulatory obligations.
High Availability & Uptime: Ensure reliability for time-sensitive clinical decisions.
EHR Integration: Embed communication within the clinical record.
Mobile Device Support: Provide accessibility where care teams work.
Nice-to-Haves: Enhancements That Can Wait
Nice-to-haves extend value once the foundation is solid. They're worth planning for, but they shouldn't drive the initial build
Advanced Analytics: Gain deeper operational and clinical insights.
AI Transcription: Reduce the burden of clinical documentation.
Extended Collaboration: Broaden coordination across care teams.
Each can meaningfully enhance the ecosystem, but only after the must-haves are reliably in place.
Applying the Framework: A Three-Question Test
These categories aren't self-evident in practice. When every stakeholder believes their request is critical, a consistent forcing function keeps prioritization objective. Before any capability lands on the must-have list, run it through three questions -- with clinical leads and IT in the same room:
-
Does a care team depend on this to do their job safely today?
-
Does the absence of this create a workaround that introduces patient risk?
-
Can this be added after stabilization without disrupting active clinical workflows?
If the answer to Question 1 or Question 2 is yes, it's a must-have. If the honest answer is only Question 3, it defers to Phase 2.
The discipline here is in the room, not the framework. Clinicians tend to anchor on Question 1; IT tends to anchor on Question 3. Requiring both groups to answer all three -- out loud, together -- surfaces the assumptions that produce scope creep before they get embedded in a requirements document.
Why the Distinction Matters
Separating must-haves from nice-to-haves keeps the initiative anchored to what strategic planning is really about: prompt decisions, fluid coordination, and consistent patient care.
It sets realistic expectations and ensures every dollar goes toward closing the communication gaps behind nearly a third of malpractice claims, not toward features that impress in a demo but never touch the bedside.
⚠️ Case in Point: The NHS and Microsoft Teams
When the NHS accelerated its Teams rollout during COVID-19, adoption surged overnight while governance and workflow integration lagged behind. Clinicians began sharing patient identifiers, images, and clinical questions over Teams chat because it was faster than sanctioned tools — forcing trusts to issue formal guidance that Teams chat was not an approved clinical channel. The platform worked exactly as built. The workflow design didn't. UCaaS adoption had outpaced the requirements work that should have preceded it.
Workflow Design and Communication Strategy
Defining the right capabilities sets the boundary. Workflow design determines whether those capabilities actually get used — and that's where most UCaaS rollouts lose momentum.
You don't need a perfect map before you move. You need enough clarity to take the next step without rebuilding yesterday's problems inside tomorrow's platform. Good enough to start is better than perfect too late.
Begin with two questions directed at charge nurses and shift leads — not IT:
- Which workflows are load-bearing? These support safe care and need to survive the transition intact.
- Which are workarounds? These exist because current systems fall short and should disappear when a better tool arrives.
That conversation, even informal, surfaces more actionable signal than a formal requirements workshop — and it gets you moving.
Next, assign channels a clear role. Not exhaustively — just enough to eliminate the most common failure mode: clinicians defaulting to whatever feels fastest. A working starting point:
- Voice or alert for anything requiring an immediate response
- Secure message for urgent but non-immediate clinical questions
- Async message for routine updates and coordination
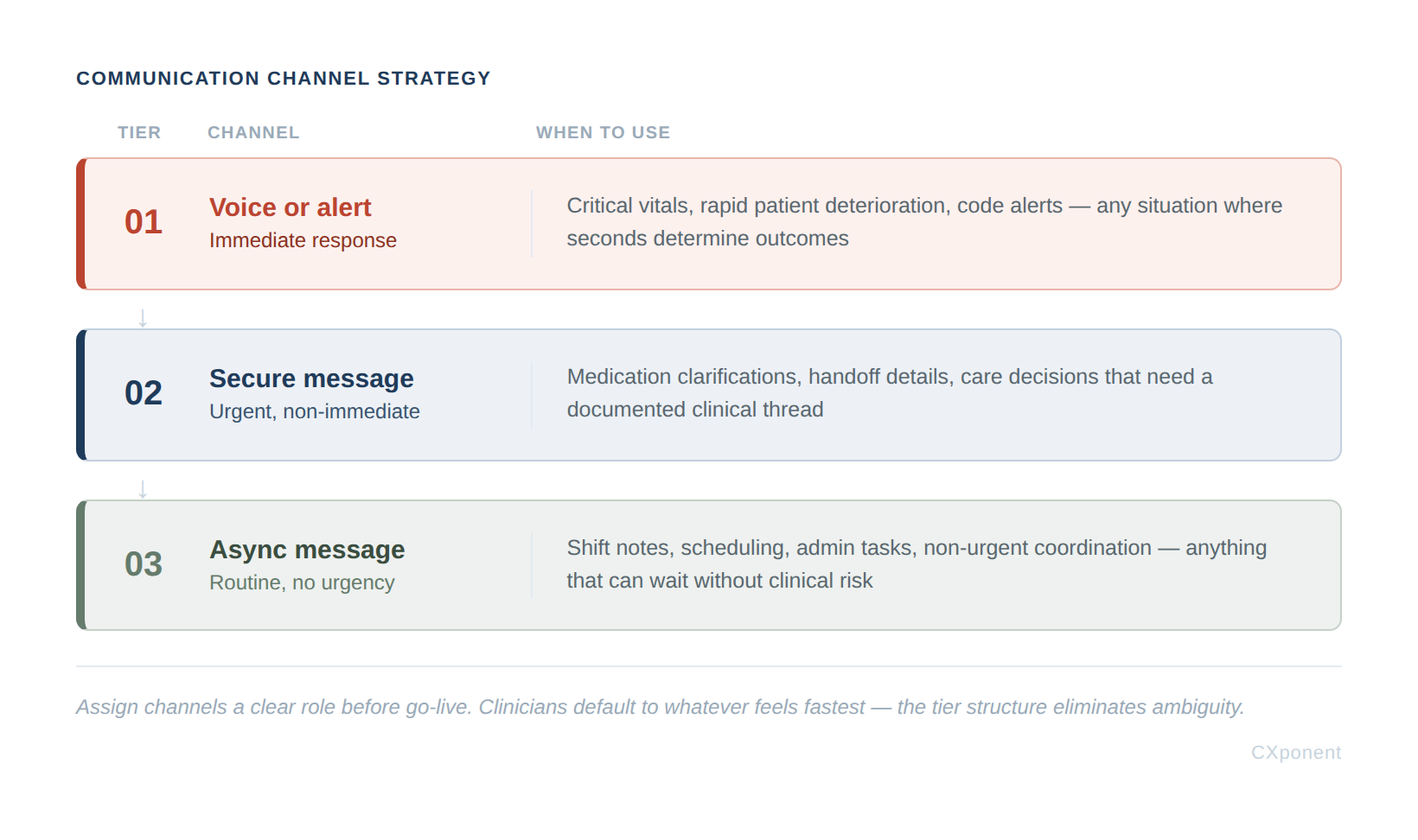
This doesn't need to be final. It needs to be functional. Refine it as the rollout matures and real usage patterns emerge.
Last, name one person responsible for channel discipline post-go-live before configuration begins. Not a committee — one person. Governance doesn't need to be elaborate at this stage; it needs to exist. Someone to hold the line, absorb the edge cases, and make the calls that keep the design from drifting. That role can evolve. Right now, it just needs to be filled.
Prioritizing EHR Integration
A well-designed channel strategy moves the right message to the right person at the right time, but in healthcare, "right" also means in context. A secure message about a deteriorating patient loses most of its value if the clinician has to leave the chart to read it. Communication only becomes clinically useful when it lives inside the patient's record.
That's why EHR integration can't be treated as a later-phase nice-to-have. Whether the environment runs on Epic, Cerner, Meditech, Allscripts, athenahealth, eClinicalWorks, NextGen, or Greenway, the communication platform has to meet clinicians where they already work. Without that integration, messaging drifts into a parallel universe, resulting in it to be siloed from the chart, disconnected from orders, and forcing nurses and physicians to carry the cognitive load of tying messages to patients in their heads. Context dies in a thread instead of landing in the chart.
The Optimal EHR Integration:
- Native connector exists for your EHR, or a robust middleware with active development
- Messages anchor to patient encounter, not just contact record
- Alerts surface inside the clinical workflow, not a separate application
|
💡 Don't wait for perfect integration to move forward — but know exactly what you're trading off. Document every gap, assign an owner, and set a resolution deadline before go-live. A known gap with a plan is manageable. A surprise on day one is not. |
One unresolved item on this list is a day-one workaround waiting to happen. Two unresolved items is a go-live risk.
The goal is the opposite: communication embedded in the workflow and accessible at the point of care. When messaging, voice, and alerts surface inside the EHR; anchored to the right encounter, order, and team—the platform stops being a separate tool and starts behaving like part of the clinical record itself.
Gap Analysis: The Final Validation Before Implementation
Gap analysis is the critical, final validation before execution. By comparing current-state workflows with future-state design, this analysis surfaces risks like missing integrations and unaccounted-for process dependencies, while they are still cheap to fix and before go-live decisions are locked.
Three categories cover the gaps that most commonly derail go-live:
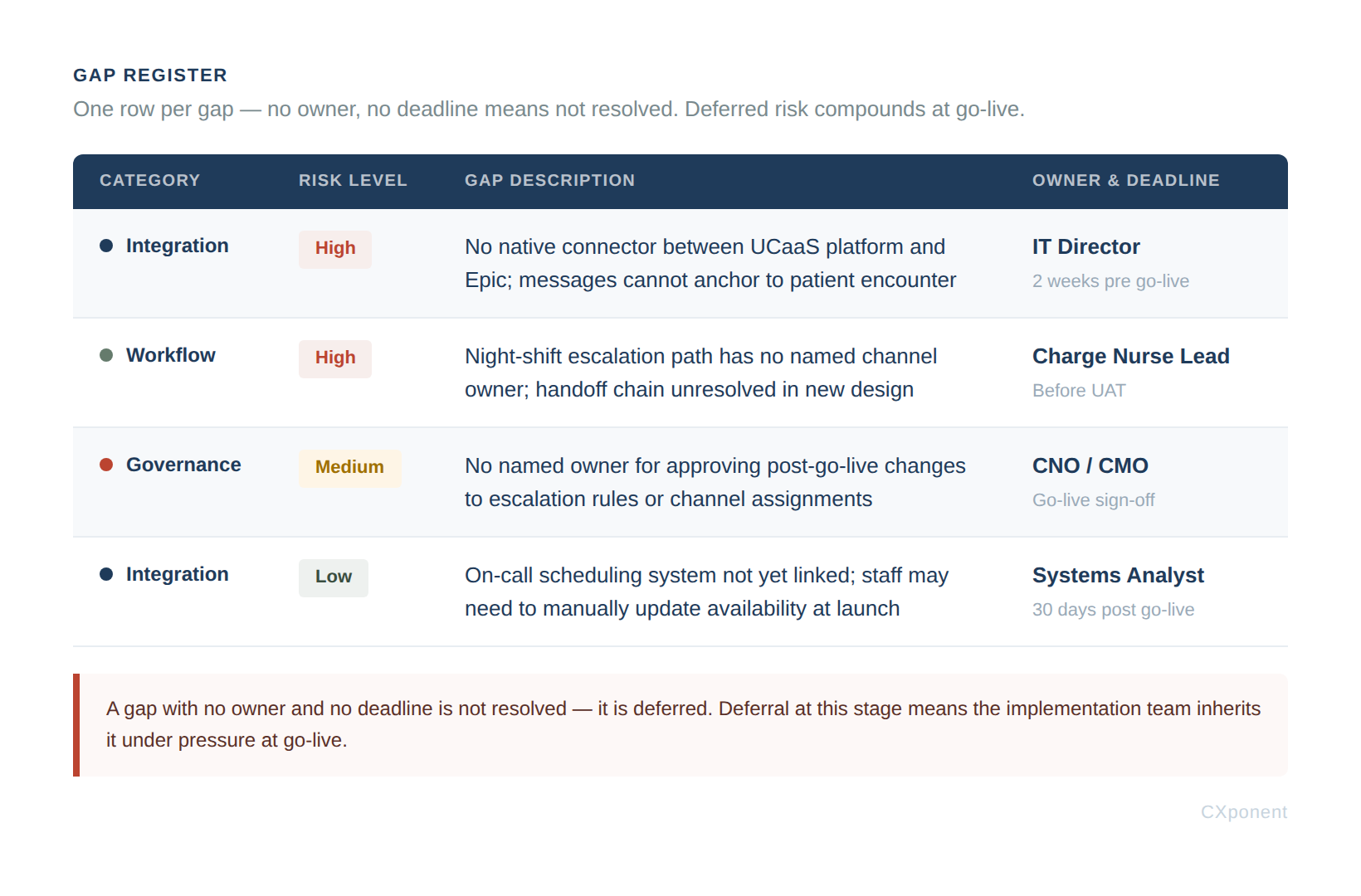
Integration Gaps – Where the new platform does not connect cleanly to existing systems: EHR, scheduling, on-call management, overhead paging. Each unresolved integration is a workaround waiting to be invented.
Workflow Gaps – Mapped workflows that have no clear channel owner or escalation path in the new design. If the tabletop exercise from Workflow Design surfaced unresolved handoffs, they land here.
Governance Gaps – Decisions that have no named owner. Who approves changes to escalation rules after go-live? Who resolves disputes between IT and clinical ops? Unnamed ownership is a gap as much as a missing integration is.
The output is a gap register: one row per gap, with four fields: category, risk level, owner, and resolution deadline. This is the artifact that gates go-live authorization. If a gap has no owner and no deadline, it is not resolved -- it is deferred, and deferral at this stage means the implementation team inherits it under pressure.
Left unresolved, these gaps become day-one workarounds that quickly erode clinician trust. Catching them here prevents the rework and delays that derail a sound strategy. This final disciplined step determines whether the rollout will be coherent or chaotic, setting the definitive stage for execution.
The Pivot Point: Planning to Execution
Step back, and the arc of this phase comes into focus. Discovery mapped the current state—how communication actually moves today, where it breaks down, and what clinicians work around to get through a shift. Planning defines the future state, the deliberate design of how people, workflows, and technology will operate together once the new system is live. Everything covered here, from stakeholder alignment to channel strategy, EHR integration, and gap analysis, exists to make that future state real rather than aspirational.
The quality of that planning work is what separates a rollout that lands from one that fragments on contact with the floor. When the future state is clearly defined, adoption follows because the system meets clinicians inside the workflows they already use. Friction drops because messages, escalations, and handoffs travel the paths the work actually takes. And patient outcomes improve, and not because a new tool was installed, but because the right information reached the right person at the moment a decision had to be made.
That is the handoff point. Planning has set the destination, the route, and the guardrails; execution is where the organization actually makes the trip. Part 3 picks up with implementation and deployment. Translating the future-state design into configured systems, trained teams, and a go-live that holds together under real clinical pressure.
Strategic planning provides the clarity needed to ensure implementation teams aren't making foundational decisions under go-live pressure. If the following checklist is complete, the organization is ready to transition to implementation.
Before moving to Part 3, confirm you have the following in hand:
-
Requirements matrix reviewed and signed off by clinical, operational, and IT leads
-
Communication tier assignments documented and validated with clinical staff
-
EHR integration confirmed with vendor on a native connector, not a custom engagement, or a middleware solution with confirmed mitigation of the gaps
-
Workflow design validated
-
Gap register complete with category, risk level, owner, and resolution deadline for every open item
If any item on this list is incomplete, unresolved, or still pending sign-off, stop here. Part 3 assumes a stable, validated foundation and gaps carried forward don't close on their own; they compound. Get the sign-offs, resolve the open items, and confirm the integration path before proceeding. What follows is implementation, and implementation has no patience for unfinished design.
About the Author
Tony Tobias
Tony Tobias is an EX/CX consultant dedicated to helping organizations build stronger connections between their employees, customers, and communities. With a passion for improving the moments that matter most across the employee and client journey, Tony works with teams to design practical strategies that elevate engagement, strengthen culture, and drive meaningful business outcomes. Outside of his professional work, Tony’s life is deeply rooted in family and friends. With his son and daughter being heavily involved in youth sports, Tony and his wife, Meredith, spend much of their time supporting, coaching, and cheering from the sidelines. Through this involvement, Tony values the lessons youth athletics teach, such as teamwork, resilience, leadership, and character—principles that also influence how he approaches his work with organizations and teams.
Need help navigating your technology decisions?
Our advisory team helps you evaluate, negotiate, and implement — at no cost to you.
Talk To Us